 Skip to content
Skip to content 

Key Take Home Points
• Preserving the lateral meniscus is key due to rapid progression to early OA if left untreated
• Prompt onwards referral for younger patients +/- mechanical symptoms e.g. locking suggesting bucket handle tear
particularly where lateral meniscal injury is suspected
• Always have a high index of suspicion in younger patients presenting with meniscal symptoms of concomitant ligament
injury
• Degenerative meniscal tears rarely need surgery (at least 3 months of high-quality rehab prior to considering onward
referral)
The Big 5 – Acute Swelling – Haemarthrosis
1) Fracture #
2) Extensor mechanism injury (quads/patella tendon rupture)
3) ACL
4) Large meniscal tear (outer red zone aka vascular zone)*
5) Patella dislocation
*Less vascular structure vs cruciate ligament = slower onset swelling response typically
** Red herring – patient on anticoagulants
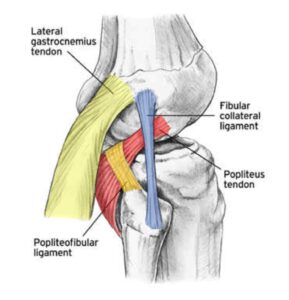
Posterolateral Corner
- Popliteus tendon
- Popliteofibular ligament
- LCL
Relevant Research / Guidelines
Kise et al (2016) – Exercise therapy versus arthroscopic partial meniscectomy for degenerative meniscal tear in middle aged patients: randomised controlled trial with 2-year follow-up
Siemieniuk et al (2017) – Arthroscopic surgery for degenerative knee arthritis and meniscal tears: a clinical practice guideline
Lowery et al (2006) – Clinical Prediction Rule for Meniscal Assessment
NICE Guidelines – McMurray’s test is no longer recommended as per NICE guidelines & BMJ Best Practice Review with moderate diagnostic accuracy Smith, 2015; Decary, 2017)
![]()
![]()
